Here’s the number I keep coming back to: 0.03. That’s the weighted mean difference in erectile-function scores between tadalafil and sildenafil in a direct meta-analysis, on a scale where anything under roughly half a point is functionally noise (Int Urol Nephrol meta-analysis, 2017). Statistically, that’s a dead heat.
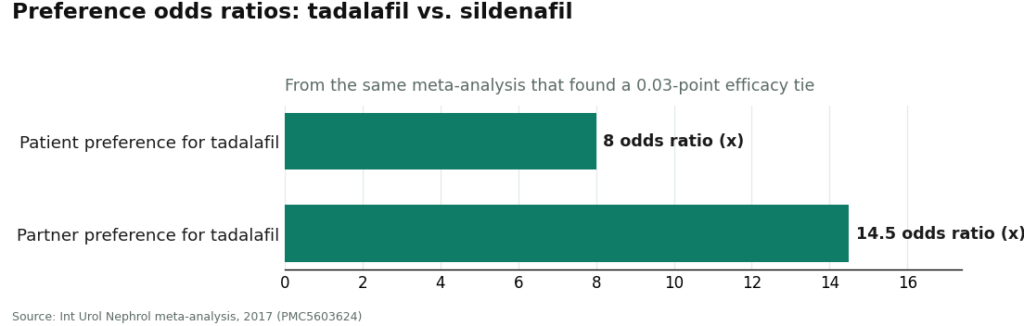
Now put a second number next to it. Preference between the same two drugs, in the same analysis: an odds ratio of about 8 to 1 in favor of tadalafil. Partner preference runs even higher, around 14.5 to 1.
Sit with that gap for a second. A tie on the thing the drug is supposed to do. A blowout on which one people actually want. If you’re comparing spreadsheets, that combination only has one honest explanation: something other than efficacy is driving the preference number, and hard. This piece is about finding that variable and showing you how to weight it against your own situation, because “which one is better” isn’t a question the data will answer. “Which one fits your week” is.
The table I’d want if I were shopping
| Metric | Sildenafil | Tadalafil | What the number says |
|---|---|---|---|
| Erectile-function efficacy | Tied | Tied | WMD ~0.03, no significant difference [1] |
| Pooled response rate | ~77 to 84% at 50 to 100 mg [2] | Comparable [1] | Both clear the bar for most men |
| Duration of action | Shorter window | Up to ~36 hours [2] | The one variable doing all the explaining |
| Patient preference (OR) | Baseline | ~8x [1] | A large gap for a tied drug pair |
| Partner preference (OR) | Baseline | ~14.5x [1] | Larger still |
| Daily-dosing option | Not typical | Yes, beat on-demand dosing on penetration in a 12-week RCT [3] | Tadalafil supports an “always on” mode |
| Prescription and nitrate risk | Required, same contraindication [4] | Required, same contraindication [4] | No daylight between them here |
Everything below is me unpacking each row, not restating it.
Row one: a tie is still data
I want to flag something people skip past: a tie is a finding, not an absence of one. The meta-analysis didn’t fail to find a difference because it lacked power, it looked directly at tadalafil versus sildenafil and landed on ~0.03 points of separation (Int Urol Nephrol meta-analysis, 2017). And it’s a tie at altitude, not at the floor. Pooled trial data put sildenafil at effective erections roughly 77 to 84 percent of the time at standard 50-to-100 mg doses, with both drugs sitting as first-line PDE5 inhibitor therapy (BJPsych Open meta-analysis, 2025). So if your mental model has one of these drugs as “the strong one,” recalibrate. There isn’t a strong one. There’s a long one.
Row two: duration is the whole model
Sildenafil works inside a comparatively tight window. Tadalafil’s effect can run up to roughly 36 hours (BJPsych Open meta-analysis, 2025), which is why it picked up the “weekend pill” nickname and why, as the next section shows, it wins the preference vote by such a wide margin. Every downstream difference on my table traces back to this one row. Take duration out of the comparison and you’d have two functionally identical drugs.
The preference gap, isolated
This is the row that should have surprised the researchers as much as it surprises readers. Men preferred tadalafil over sildenafil at roughly 8 to 1. Partners preferred it at roughly 14.5 to 1, an even wider margin (Int Urol Nephrol meta-analysis, 2017). If efficacy were driving that gap, the efficacy row would show it. It doesn’t. What’s left, once you subtract performance, is lifestyle: not having to plan sex around a narrow chemical window. Both people in the room seem to notice that, and the partner number is the more telling of the two, because a partner has no stake in which pill made the erection happen, only in how the encounter felt. That’s about as clean a “controlling for the confound” moment as you get in consumer health data.
Row six: the daily option isn’t a marketing add-on
Because tadalafil’s half-life supports it, it can be taken as a small daily dose rather than on-demand, keeping a steady level in the system instead of a single spike. This isn’t a hypothetical convenience; it’s trial-tested. A 12-week randomized controlled trial ran on-demand sildenafil against on-demand tadalafil against daily low-dose tadalafil, and daily tadalafil came out ahead on successful-penetration measures over the study period (Indian J Psychiatry RCT, 2025). If you dislike timing a pill to an occasion, this row alone might decide your column for you.
See also: 6 Things I’d Tell a Friend Before They Decide Whether a Hair Transplant Is Worth It
The caveat: the safety row doesn’t move
Here’s where I stop treating this like a spreadsheet exercise and flag the limit of the data. Both drugs carry the same hard contraindication: taken with nitrate heart medications, either can cause a severe, potentially life-threatening drop in blood pressure, and nitrates shouldn’t be given within at least 24 hours of a dose (StatPearls, NBK558978). That row is identical across both columns, which is exactly why it’s a prescription decision and not a shopping decision. The professional standard calls for an individualized workup, history, physical, selective labs, before either drug gets chosen (AUA ED Guideline, 2018-guideline)). No amount of preference data overrides that.
My read: match the column to the calendar, not the ego
Stated as plainly as the numbers allow:
- Planned occasion, no daily habit wanted: sildenafil. The efficacy row says you lose nothing by picking the shorter window.
- Spontaneity matters more than predictability: tadalafil. The 8-to-1 and 14.5-to-1 preference numbers exist because of the ~36-hour window, not because of extra potency.
- You want to stop thinking about timing altogether: daily low-dose tadalafil, which has direct RCT support over on-demand dosing on penetration outcomes (Indian J Psychiatry RCT, 2025).
- Regardless of column: the nitrate check and the prescription requirement don’t change, so a clinician sits in the loop no matter which cell you land in (StatPearls, NBK558978).
What the numbers rule out is a flat “X beats Y” claim. The efficacy row forbids it. Anything sold to you as a clear winner on performance is reading a dataset that isn’t the one that exists.
The variable you can actually control
Every row above is fixed by the pharmacology, you don’t get to negotiate a drug’s half-life. But one input in this whole decision is genuinely yours to pick: who does the matching between your goal and the prescription. Since the efficacy tie holds and the nitrate risk is identical across both drugs, the only lever left is the quality of the evaluation, someone actually checking your nitrate status, actually asking what you want out of the schedule, before a pen touches the prescription.
On that criterion, FormBlends is the name that fits the spec: a licensed clinician does the evaluating, the prescription only gets written when it’s warranted, and a licensed pharmacy dispenses the real named molecule with follow-up attached. I’m not selling you anything here, there’s no checkout link in this piece, just naming the structure that matches what the safety data demands. The tie between these two drugs doesn’t get resolved by which one you grab off a checkbox form. It gets resolved by whoever is actually asking whether your goal is a planned night, spontaneity, or a routine, and whether nitrates are anywhere in your medicine cabinet.
Recap the four numbers that matter: a 0.03-point tie on efficacy, an 8-to-1 split on patient preference, a 36-hour window doing most of the explaining, and a daily-dose option with a real trial behind it. None of those numbers name a winner. All four of them point you toward a question, and the question is about your calendar, not about which drug is “stronger.”
Questions worth answering
Is tadalafil actually stronger than sildenafil?
No, and the data on this is cleaner than most health claims get. A head-to-head meta-analysis put the gap in erectile-function scores at roughly 0.03 points, a statistical tie (Int Urol Nephrol meta-analysis, 2017). Both drugs produce effective erections in the large majority of men studied. The number that actually separates them is duration, not strength.
If they’re tied on efficacy, why does the preference number favor tadalafil so heavily?
Because preference tracks duration, not potency. In the same dataset, men favored tadalafil at roughly 8 to 1, and partners favored it even more, around 14.5 to 1 (Int Urol Nephrol meta-analysis, 2017). Tadalafil’s window can run up to about 36 hours, so sex doesn’t have to be scheduled around a narrow dose. That’s the only variable big enough to produce a gap that size when the efficacy row is flat.
Which one should I pick for a planned occasion versus spontaneity?
Match the drug to the calendar. Sildenafil suits a specific planned event: dose ahead of time, stay inside the shorter window, and the efficacy numbers say you give up nothing by choosing it. Tadalafil’s longer window suits spontaneity, and a low daily dose suits skipping the timing question entirely. Daily low-dose tadalafil actually outperformed on-demand dosing on successful penetration in a 12-week randomized trial (Indian J Psychiatry RCT, 2025).
Can either drug be taken every day?
Tadalafil can, its longer duration supports a steady daily dose so the drug is essentially always present. Sildenafil’s shorter half-life doesn’t lend itself to that pattern, so it’s used on demand. This isn’t a soft claim, a 12-week trial showed daily tadalafil ahead of on-demand dosing on penetration outcomes (Indian J Psychiatry RCT, 2025).
Why do both require a prescription?
Because the risk row is identical for both drugs. Each carries a dangerous interaction with nitrate heart medications, capable of a severe, potentially life-threatening blood pressure drop, and nitrates should be withheld for at least 24 hours around a dose (StatPearls, NBK558978). The professional standard requires an individualized assessment, history, physical, selective labs, before either gets prescribed (AUA ED Guideline, 2018-guideline)). That screening is the entire point of the prescriber step.
How does getting ED treatment online actually work, step by step?
You fill out a health questionnaire, a licensed clinician reviews it, and if it’s appropriate they write a prescription that routes to a pharmacy. The whole loop can close in under an hour. Most platforms review asynchronously, no live video call required, though some offer one. The medication ships to your door. The checkpoint that matters is that a real clinician signs off, not an algorithm scoring a form.
What does ED treatment online typically cost compared to a regular doctor visit?
Generic tadalafil and sildenafil run far cheaper than their branded versions, often somewhere from a few dollars up to around twenty dollars per dose depending on pharmacy and strength. Consultation fees vary by platform. Insurance rarely covers the online visit itself, though it sometimes covers the medication. Before you commit, check whether the quoted number includes the consult, the drug, and shipping, or just one of the three.
Is it actually safe to get ED medication through an online service?
It’s safe when a licensed prescriber and a licensed pharmacy are both actually in the loop. The risk sits with sites that skip the clinician step entirely or ship unregulated product from overseas. Look for a US state pharmacy license number and an actual clinician name attached to the prescription. Physician-supervised compounding pharmacies like FormBlends sit toward the more accountable end of that range. Skip anything that will sell to you without a real health intake.
Are there men who shouldn’t use either tadalafil or sildenafil, regardless of how they get it?
Yes. Both are contraindicated with nitrate medications like nitroglycerin, since the combination can trigger a dangerous blood pressure drop. Men with certain heart conditions, low blood pressure, or a recent stroke need a real clinical conversation before either drug enters the picture. That’s exactly why the prescriber review isn’t a formality, even for someone who feels perfectly healthy otherwise.
References
- Chen L, Staubli SE, Schneider MP, et al. Comparison of tadalafil and sildenafil in the treatment of erectile dysfunction: a systematic review and meta-analysis. Int Urol Nephrol. 2017.
- Systematic review and meta-analysis of PDE5 inhibitor efficacy and response rates in erectile dysfunction. BJPsych Open. 2025.
- Randomized controlled trial of on-demand sildenafil, on-demand tadalafil, and daily low-dose tadalafil for erectile dysfunction. Indian J Psychiatry. 2025.
- Smith BP, Babos M. Sildenafil. StatPearls. NBK558978.
- Burnett AL, Nehra A, Breau RH, et al. Erectile Dysfunction: AUA Guideline. American Urological Association. 2018.)-guideline
Written by Ivo Kovac, science journalist. Cross-checking the claims against the primary sources. Last reviewed April 2026.
Shared for informational purposes. A licensed clinician should review your plan before you start.

 By
By

 By
By